If you've been paying attention to the news in the United States, you know that we're seeing a lot more cases of measles than we used to. There are a few reasons for this, but one of the biggest is that more Americans are deciding not to vaccinate their kids. The problem is that parents' decision not to vaccinate tends to be based on an incomplete understanding of the purpose of vaccination. When your child gets a measles vaccine, she's protected against the disease, but she's also protecting other people against the disease. There are people who simply can't be vaccinated, either because they're too young, they're allergic, or their immune systems are weakened or suppressed. In order for them to be protected, a certain percentage of the people around them need to be vaccinated. This is called "herd immunity," and it kicks in at different percentages for different diseases. But for measles, the bar is incredibly high - any less than 95 percent vaccination, and a disease that had virtually disappeared starts coming back, and the herd (that is, us) gets sick.
Up until now, the idea of vaccinating a high enough percentage of people in every developing country to achieve herd immunity to every disease we have a vaccine for has been all but unthinkable. After all, there are so many other problems to overcome: Many vaccines have to be given in multiple doses, spaced a certain amount of time apart. Most have to be kept below or above a certain temperature (different for each disease), or they'll lose potency or even be contaminated. Furthermore, many have to be administered by a trained health professional. Put all these requirements together and you have something it‘s incredibly difficult to do consistently in developing countries, especially those where health systems are weak.
But thanks to a new vaccine-delivery technology called micro-array patches (MAPs), epidemiologists are starting to imagine the day when the population of even the poorest, most mountainous country, with the spottiest refrigeration, could have solid herd immunity to measles and other diseases like it.
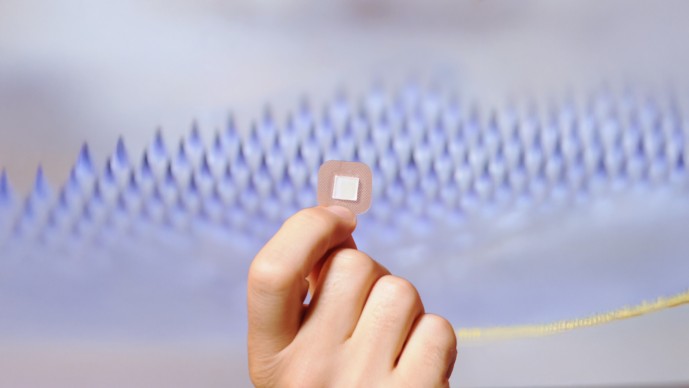
MAPs are small patches. One side of the patch looks more or less like the outside of a Band-Aid. The other side is covered in coated polymer or dissolvable projections (the researchers working on MAPs used to call these projections "needles," but that word tended to scare people for no reason, since these projections can't be seen and don't hurt). When you put the patch on your arm (or your leg, or wherever), the projections are able to reach immunologically sensitive cells in the skin's outer layer that a needle and syringe could never get to.
The potential this technology has to solve problems is huge. A vaccine given via a MAP doesn't need nearly as much protection from the cold or the heat, so it works in a country where there aren't refrigerated trucks, storage facilities, and health centers. Not only that, but since it's a patch rather than an injected vaccine, it doesn't require training to vaccinate kids - volunteers could just go house to house, slapping on patches as they go.
There are a lot of people working on MAPs, but three Grand Challenges grantees in particular stand out: Mark Prausnitz, Mark Kendall, and Michael Schrader. Interestingly, they all initially won grants through different requests for proposals with different goals. Dr. Kendall, at the University of Queensland in Australia, received a Grand Challenges Explorations (GCE) grant in 2008 focused on malaria vaccines under the challenge to create new ways of protecting against infectious diseases. Dr. Prausnitz, at the Georgia Institute of Technology, received a GCE grant in 2011 under the challenge to find new ways to accelerate, sustain, and monitor polio eradication. And Dr. Schrader, with Vaxess Technologies, won a Grand Challenges grant in 2016 focused on a polio vaccine but under the challenge to find innovative ways to manufacture vaccines.
We don't know yet how progress under these three projects will play out, but it's exciting to think of a future with multiple MAP technologies being developed in parallel, working toward a measles-rubella vaccine, with clinical trials on the horizon. When we made the initial grants we didn't know this was what we were doing, but it turns out that supporting innovation through multiple channels - different calls for proposals across the Grand Challenges family of initiatives - yielded seed funding for a whole portfolio of promising projects aiming to take MAPs to the next stage of vaccine delivery.
MAPs aren't the only vaccine delivery innovations in development - and the others are far too numerous for us to invest in them all. There are people working on aerosol vaccines that you breathe in through the nose, people working on sublingual vaccines, there are even people working on a jet vaccine that looks a little like a staple gun. I don't know what vaccine technology is going to turn out to be the most effective, but as that question gets closer to an answer, it's also getting people in poor countries a lot closer to herd immunity. Now if only we could convince the United States to follow suit.



